
Discover expertly crafted nursing care plans to provide exceptional patient care. Get step-by-step instructions and examples to enhance patient outcomes.
In healthcare, nursing care plans are indispensable tools for ensuring holistic patient care. They serve as roadmaps, guiding nurses in delivering the best possible care to their patients. In this comprehensive guide, we’ll delve into the essential components of nursing care plans examples, and explore the benefits they offer. So, let’s embark on this journey towards understanding the pivotal role of nursing care plans in healthcare.
1. Components of Nursing Care Plans

Nursing care plan guides are structured frameworks that outline the nursing care required by a patient. They encompass an individual’s unique needs, conditions, and preferences, making them invaluable to holistic patient care. These plans are designed to be patient-centered, ensuring that the care provided is not only effective but also considerate of the patient’s physical, emotional, social, and even spiritual needs.
a. Assessment:
The assessment phase involves gathering detailed patient information to identify health issues and concerns. It includes physical examinations, medical record reviews, and patient interviews to understand the patient’s condition.
b. Nursing Diagnosis:
In this stage, healthcare providers determine specific health problems. Nursing diagnoses guide interventions and can be categorized as actual, potential, or wellness diagnoses, setting the stage for effective care planning.
c. Planning:
During the planning phase, a care plan is developed to address the patient’s unique needs. It outlines interventions, strategies, and clear, prioritized care goals.
d. Implementation:
The implementation phase involves carrying out the planned interventions and documenting the care provided, ensuring attention to detail and patient comfort.
e. Evaluation:
Evaluation is an ongoing process where healthcare providers regularly assess the care plan’s effectiveness by monitoring patient progress and making adjustments as necessary to optimize outcomes.

2. Creating Comprehensive Nursing Care Plans
Nursing care plans examples come in various types, including informal, formal, standardized, and individualized plans. Each has its unique purpose and application:
- Informal Care Plans: Informal care plans are unrecorded and exist within a nurse’s mind. They are used for spontaneous decision-making during a shift, relying on a nurse’s experience and quick thinking to address immediate patient needs.
- Formal Care Plans: Formal care plans are structured and documented plans that are typically part of a patient’s medical records. They provide a comprehensive roadmap for care, ensuring accountability and continuity of care.
- Standardized Care Plans: Standardized care plans are pre-established protocols for groups of patients with common healthcare needs. While they offer efficiency, they may not always address individual patient requirements.
- Individualized Care Plans: Individualized care plans are tailored to each patient’s unique health conditions, preferences, and circumstances. They prioritize a personalized, patient-centered approach to care.
3. Nursing Care Plan Examples

To illustrate the practical application of nursing care plan guides, let’s delve into specific examples that demonstrate how they are tailored to address various patient needs:
a. Pain Management Care Plan:
Objective: To address pain relief strategies for patients dealing with chronic or acute pain.
- Assessment: Begin with a thorough assessment of the type and intensity of the patient’s pain, its location, and any factors that exacerbate or alleviate it. Consider using pain scales to measure pain levels.
- Nursing Diagnosis: Identify the specific pain-related issues, such as the patient’s inability to communicate pain, or discomfort due to an injury or surgical procedure.
- Planning: Develop a comprehensive pain management plan, which may include medication administration, physical therapy, relaxation techniques, and patient education. Set clear goals for pain reduction or management.
- Implementation: Administer pain-relief medications as prescribed, assist with positioning and mobility to minimize pain, and educate the patient on pain management techniques.
- Evaluation: Continuously assess the patient’s pain levels, monitor the effectiveness of pain management interventions, and adjust the plan as needed to provide optimal relief.
b. Wound Care Plan:
Objective: Detail the treatment and care of wounds, promoting wound healing and preventing infection.
- Assessment: Examine the wound’s size, type, and appearance. Assess surrounding skin for signs of infection or irritation. Evaluate the patient’s overall health to determine their ability to heal.
- Nursing Diagnosis: Diagnose specific wound-related problems, such as the risk of infection, impaired tissue healing, or complications due to comorbidities.
- Planning: Develop a wound care plan that includes wound cleansing, dressing changes, and measures to prevent infection. Set healing goals and document the characteristics of the wound for monitoring.
- Implementation: Carry out wound care as scheduled, ensuring sterile techniques during dressing changes, and administer antibiotics or other medications as prescribed.
- Evaluation: Regularly evaluate the wound’s progress in terms of healing, infection prevention, and any changes in wound characteristics. Adjust the care plan based on the wound’s response to treatment.
c. Medication Administration Care Plan:
Objective: Manage medication schedules, ensure patient compliance, and monitor potential side effects.
- Assessment: Review the patient’s medication history, allergies, and any known adverse reactions. Assess the patient’s ability to self-administer medications and any cognitive impairments.
- Nursing Diagnosis: Identify medication-related issues, such as non-compliance, potential drug interactions, or side effects.
- Planning: Develop a medication administration plan, specifying the schedule, dosage, and route for each medication. Educate the patient about their medications and potential side effects.
- Implementation: Administer medications as prescribed, ensuring the patient follows the correct schedule. Monitor for adverse reactions, and document medication administration.
- Evaluation: Continuously assess the patient’s response to medications, check for side effects, and evaluate whether the patient is adhering to the prescribed regimen. Adjust the plan as needed to ensure safe and effective medication management.
d. Nutritional Plans Care Plan:
Objective: Design dietary plans for patients with specific dietary needs, such as those with dietary restrictions or nutritional deficiencies.
- Assessment: Evaluate the patient’s dietary requirements based on their medical condition, allergies, preferences, and restrictions. Assess the patient’s weight, BMI, and nutritional status.
- Nursing Diagnosis: Diagnose specific nutritional concerns, like malnutrition, weight loss, or dietary non-compliance.
- Planning: Develop a nutritional plan tailored to the patient’s dietary needs. This may include dietary modifications, nutritional supplements, and education about healthy eating habits. Set goals for weight maintenance or gain.
- Implementation: Ensure the patient receives the recommended diet, assist with meal planning and preparation, and provide nutritional education. Monitor the patient’s food intake and document their dietary progress.
- Evaluation: Regularly assess the patient’s nutritional status, weight changes, and adherence to the dietary plan. Adjust the plan to address any nutritional deficiencies or changes in dietary requirements.
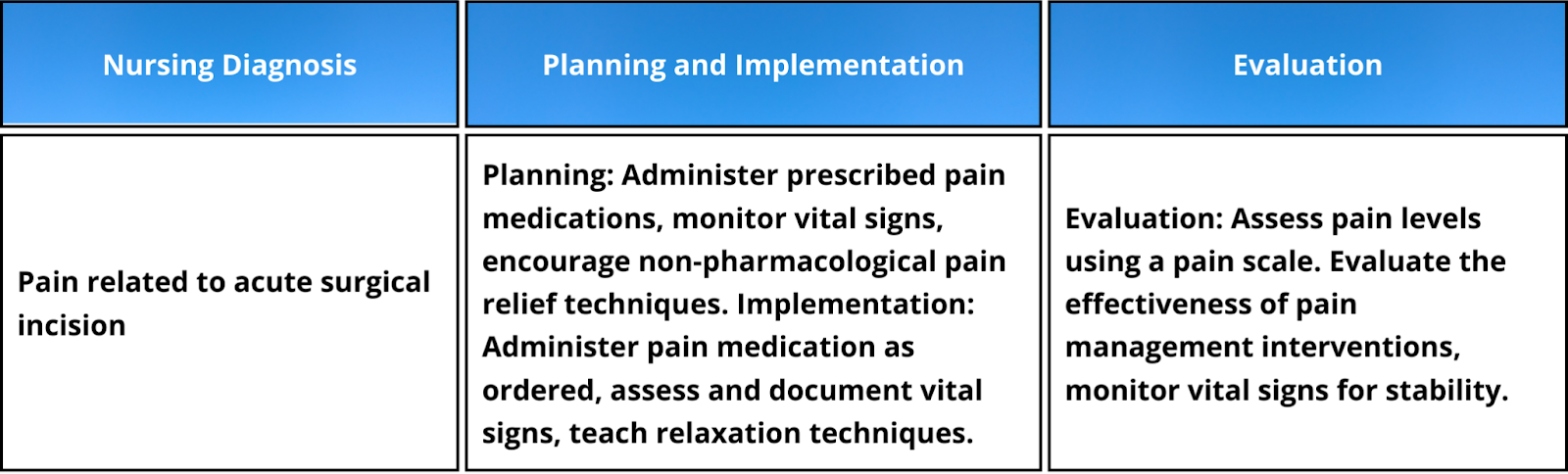
e. Nursing Care Plan Three-Column Format
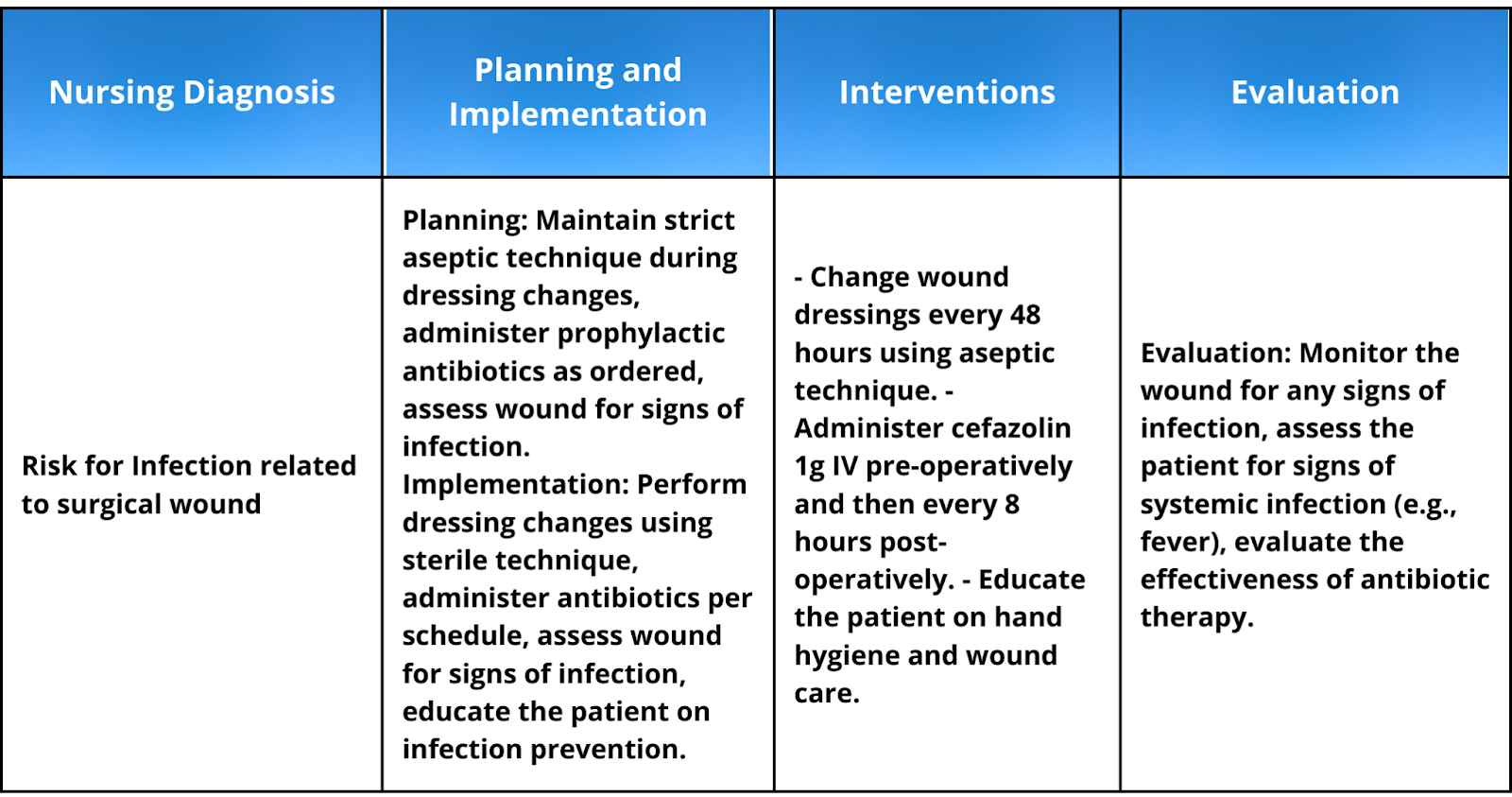
f. Nursing Care Plan Four-Column Format
4. Implementing and Evaluating Care Plans
The effectiveness of nursing care plan guides lies not only in their creation but also in their implementation and continuous evaluation. Here, we’ll explore how care plans are put into action and why ongoing assessment is vital for optimizing patient care. Nursing care plans guide the systematic and patient-centered delivery of healthcare, ensuring that each aspect of a patient’s well-being is addressed.
Implementing Care Plans:
Implementing a care plan involves putting the documented interventions into practice. It’s a critical phase that demands precision and collaboration among the healthcare team. The following steps are involved in the implementation process:
- Execution of Planned Interventions: Nurses and other healthcare professionals carry out the interventions outlined in the care plan. These may include administering medications, providing wound care, or offering emotional support.
- Documentation: Detailed and accurate documentation of care provided is crucial. This documentation not only ensures transparency and accountability but also serves as a valuable reference for the healthcare team.
- Communication: Effective communication among team members is vital. Nurses collaborate with other healthcare providers, such as physicians, therapists, and social workers, to ensure that all aspects of patient care are addressed.
Evaluating Care Plans:
Evaluating care plans is an ongoing process that helps gauge their effectiveness and make necessary adjustments. This phase is essential because patients’ needs and conditions can change over time. Here’s how the evaluation process works:
- Regular Assessment: Care plans are not static; they must adapt to the patient’s evolving needs. Regular assessments involve reevaluating the patient’s health status and comparing it to the care plan’s goals.
- Adaptation: Based on the assessment results, care plans are adopted. This may involve changing interventions, setting new goals, or discontinuing certain actions if they are no longer necessary.
- Monitoring Patient Progress: Continuous monitoring ensures that the patient’s progress aligns with the care plan’s objectives. Any discrepancies or issues can be addressed promptly.
- Outcomes and Adjustments: The final step in the evaluation process is to measure the outcomes of care. If the patient’s health improves as intended, the care plan is considered successful. If not, adjustments are made to improve patient outcomes.
5. Benefits of Nursing Care Plans

Nursing care plan guides are not just paperwork; they are dynamic tools that bring about a host of advantages, benefiting both healthcare providers and their patients. Here’s a deeper look at the benefits they offer:
a. Improved Patient Care:
Nursing care plans prioritize the patient’s well-being above all else. Care plans ensure that no aspect of care is overlooked by systematically outlining the patient’s unique needs and the actions required to address them. This approach helps nurses deliver comprehensive, patient-centered care, improving patient outcomes.
b. Enhanced Communication Among Healthcare Providers:
In a healthcare setting, collaboration is critical. Formalized care plans provide a clear and structured framework for communication and coordination among healthcare providers. Physicians, nurses, therapists, and other professionals can easily understand the patient’s care goals and actions, ensuring that everyone is on the same page regarding patient management.
c. Better Patient Outcomes:
The primary goal of nursing care plans is to enhance patient outcomes. By setting specific, measurable, and achievable care goals, and regularly evaluating progress, care plans enable healthcare providers to make informed decisions. This approach leads to better patient care and a higher likelihood of positive health results.
d. Patient and Family Involvement:
In creating individualized care plans, healthcare providers often involve patients and their families in decision-making. This collaboration empowers patients to actively participate in their care, express their preferences, and understand their treatment. It fosters a sense of control and partnership in healthcare, which can contribute to improved patient experiences.
e. Legal Documentation and Accountability:
Formal care plans serve as legal documentation, providing a record of the care and the decisions made. This documentation is essential for accountability and liability purposes. In disputes or legal matters, care plans offer a transparent and documented history of the care provided.
f. Streamlined Workflow:
Standardized care plans, in particular, can enhance efficiency in healthcare settings. They offer a set of pre-established protocols for routine procedures and conditions, reducing the time required to create individual care plans from scratch. This streamlined workflow can be especially beneficial in busy healthcare environments.
g. Research and Quality Improvement:
Care plans play a role in data collection and research in healthcare. The information gathered from care plans can be analyzed to assess the effectiveness of specific interventions or care strategies. This, in turn, contributes to the continuous improvement of healthcare quality and practices.
6. Conclusion
In healthcare, nursing care plans serve as the compass that guides healthcare providers toward delivering holistic patient care. They are not just documents but crucial tools that help nurses and the entire healthcare team provide effective, patient-centered care.
7. FAQ

What Should Be Included in a Nursing Care Plan?
A nursing care plan should consist of these essential components:
- Health Assessment: A comprehensive evaluation of the patient’s physical and psychological health, including vital signs, medical history, and current condition.
- Nursing Diagnosis: Identifying health issues based on the assessment, guiding the direction of care.
- Planned Interventions: Specific actions or treatments aligned with the nursing diagnoses and the patient’s needs.
- Schedule for Evaluation and Adjustment: A timeline for assessing progress and making necessary plan adjustments.
How often should a nursing care plan be updated?
Nursing care plans should be updated regularly, with at least one update per shift. However, more frequent updates may be necessary for significant changes in the patient’s condition or healthcare needs.
How important is a nursing care plan?
A nursing care plan is of utmost importance in healthcare. It guides healthcare providers in delivering comprehensive, patient-centered care by systematically addressing health assessments, nursing diagnoses, interventions, and evaluation schedules. This structured approach improves patient care, fosters better communication among healthcare providers, and leads to superior patient outcomes. Additionally, care plans serve as crucial legal documents, enhance patient empowerment, and are fundamental to modern healthcare practice.